Sometimes an old injury flares up, and usually at the worst possible moment. It might be a tendon that just won’t heal, a joint that gets inflamed every three months, or even a shoulder that keeps acting up. It’s precisely these situations that push people to look beyond traditional rehabilitation and turn their attention to healing peptides.
In virtually every serious discussion about recovery peptides, two compounds are mentioned: BPC-157 and TB-500. Both are backed by serious scientific research, which is why they’re often compared as if you have to choose one or the other. In doing so, people overlook the more important question of what each one actually does and when it makes sense to use them.
In this article, we’ll help you understand their mechanisms of action, research, dosages, and side effects, and provide honest recommendations on when to take them separately, when to combine them, and which format is best suited to which purpose.
What Is TB-500? Understanding the Healing Powerhouse
What is TB-500 at the molecular level? It’s a synthetic peptide fragment derived from Thymosin Beta-4 – a naturally occurring protein found in virtually every cell of the human body. The specific fragment is the actin-binding domain: the portion of Thymosin Beta-4 responsible for regulating actin polymerization and, critically, for driving cell migration.
That actin mechanism is what makes TB-500 different from most healing peptides. Most repair compounds work by signaling the body to do something – produce more collagen, reduce inflammation, stimulate growth factors. TB-500 works by actively recruiting cells to the site of damage. It doesn’t just tell the body to repair; it mobilizes the cellular workforce and moves it to where the work needs to happen.
The downstream effects of this mechanism are significant: angiogenesis (formation of new blood vessels into damaged tissue), accelerated wound closure, collagen synthesis, and stem cell mobilization. This is why TB 500 peptide has been used extensively in equine veterinary medicine for decades – racehorses with tendon and soft tissue injuries respond to it reliably, and that long track record in a high-performance animal population is part of why human research interest has been so persistent.
TB-500 is a research compound, not an FDA-approved medication. Any protocol using it is operating in research territory.
TB-500 Benefits: What the Research Shows
TB 500 benefits are rooted in a mechanism that’s been studied at a serious scientific level, including in landmark peer-reviewed journals.
Bock-Marquette et al. published a foundational study demonstrating that Thymosin Beta-4 activates integrin-linked kinase and promotes cardiac cell migration, survival, and cardiac repair following injury. This was the paper that put TB-4 and its derivatives on the map for tissue repair research, demonstrating not just that the compound had biological activity, but also the specific molecular pathway (ILK activation) through which it drives cellular migration and survival.
Goldstein et al.’s comprehensive review cataloged TB-500’s multifunctional activity across wound healing, angiogenesis, inflammation reduction, and stem cell mobilization. The review covers both the basic biology and the clinical application landscape – it’s the most complete single source on what this compound actually does and why.
Practically, what TB 500 delivers: accelerated tendon and ligament repair, improved healing in muscle fiber tears, reduced chronic inflammation at injury sites, enhanced wound closure and skin regeneration, and, notably, cardiac tissue support in post-injury contexts. The systemic nature of its action distinguishes it from more localized healing peptides: TB-500 travels throughout the body rather than acting primarily at the injection site, making it particularly valuable for multi-site or hard-to-localize injuries.
Hair growth support has been reported in research and community reports, attributed to stem cell mobilization in follicular tissue. It’s a secondary benefit rather than a primary mechanism, but it shows up consistently enough to be worth noting.
TB-500 Side Effects: What to Watch For
TB 500 side effects reported in the research and user community are generally mild, which is part of why it’s become a go-to in serious recovery protocols.
Most common: temporary fatigue or mild head fog during the loading phase, particularly in the first week. Injection site irritation – redness or a small welt – is standard and resolves quickly. Some users report brief headaches or mild flu-like symptoms in the first few days. These typically pass as the body adjusts.
The one contraindication worth flagging clearly: because TB-500 promotes angiogenesis, anyone with active cancer or unresolved tumors should avoid it. Increased blood vessel formation in that context is a theoretical risk that isn’t worth taking. This isn’t a common scenario in the research community, but it’s a non-negotiable consideration.
The other thing that looks like a side effect but usually isn’t: an impure or contaminated product from unverified sources can cause reactions that are attributed to the compound. Third-party testing is directly relevant to the side effect profile. Our TB-500 vials are batch-tested by Freedom Diagnostics with COAs published by lot number – what’s on the label is what’s in the vial.
BPC-157 vs TB-500: How They Compare
The comparison between TB 500 and BPC-157 is most useful when framed in terms of mechanism rather than outcome.
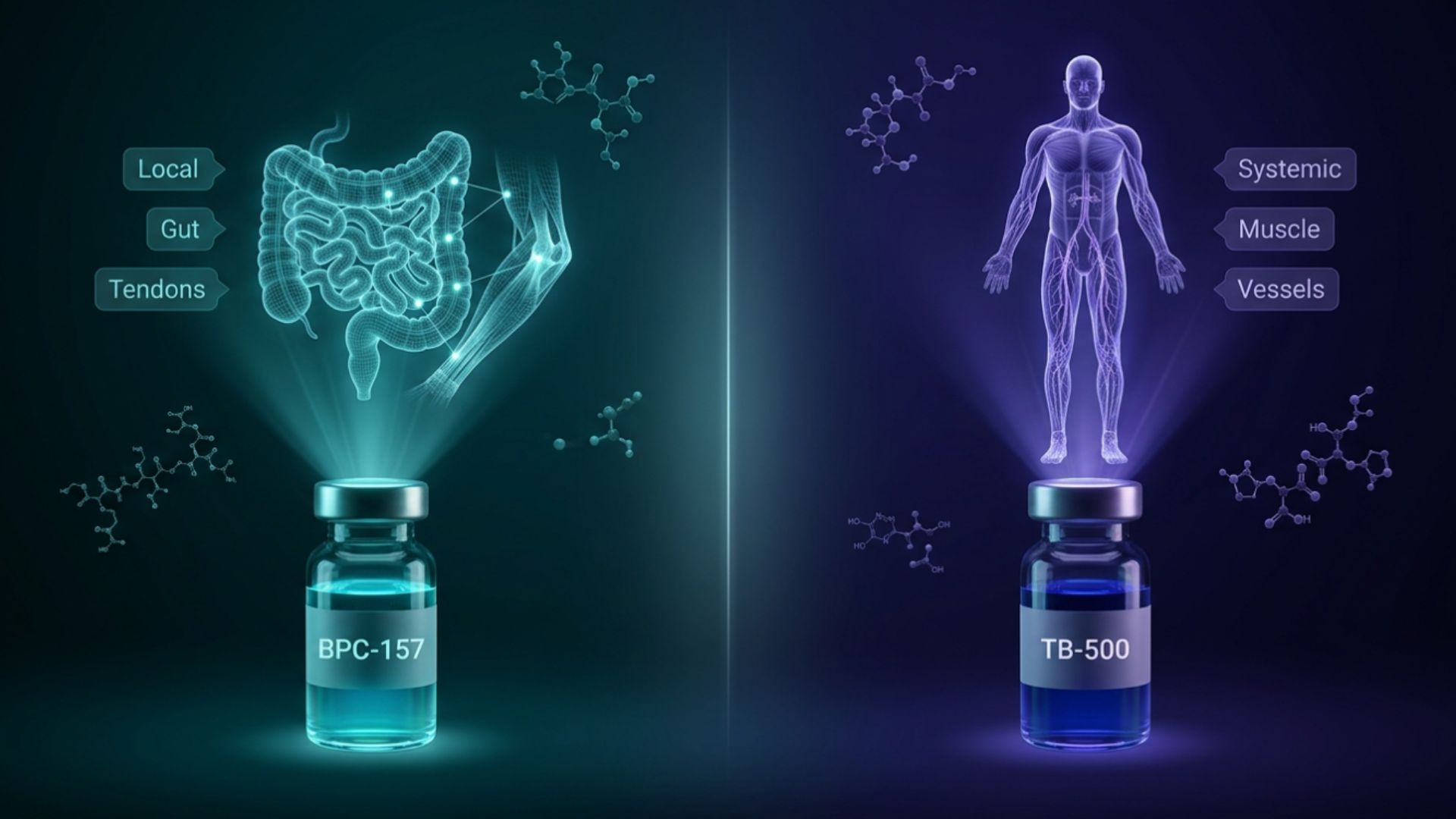
BPC-157 is a synthetic pentadecapeptide derived from a protein found in human gastric juice. Its repair activity is concentrated: it works through growth factor pathways, nitric oxide signaling, and direct tissue-protective effects, with particular strength in gut mucosa, tendons, and ligaments. Chang et al. documented BPC-157’s promotion of tendon outgrowth, cell survival, and migration in tendon healing models – the localized repair signal is consistent and well-characterized.
TB-500 acts systemically. It recruits cells from the broader circulatory pool and directs them to damage sites. Where BPC-157 is fixing the specific injury, TB-500 is building the vascular and cellular infrastructure around it.
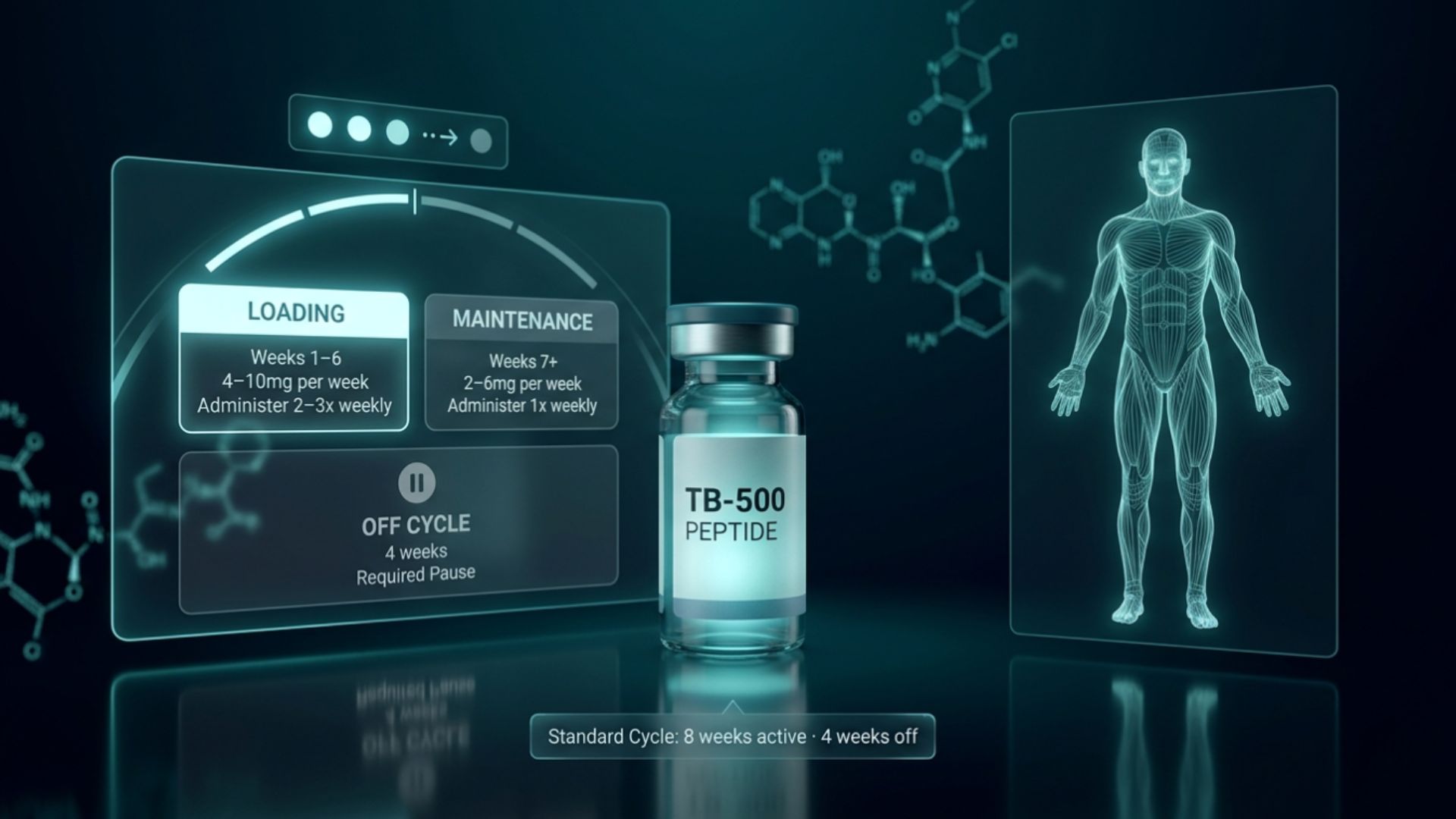
Half-life and dosing cadence differ significantly. BPC-157’s shorter half-life means daily subcutaneous injections are standard. TB-500’s longer half-life supports a loading/maintenance model – multiple injections per week during loading, then dropping to weekly or less during maintenance.
For acute, localized injuries – gut issues, specific ligament tears, tendon problems – BPC-157 is often the more targeted starting point. For chronic injuries, multi-site issues, or tissue with compromised circulation (where the problem is partly that the body can’t deliver repair resources to the damage), TB-500’s systemic cellular migration mechanism fills the gap that BPC-157 alone can’t reach.
BPC 157 and TB 500 Together: The “Wolverine Stack” Explained
BPC 157 and TB 500 combined are called the Wolverine Stack in research and biohacking communities, and the name stuck because it captures something real about what happens when you run both simultaneously.
BPC-157 delivers a localized repair signal, accelerating tissue healing at the site, protecting gut mucosa, and stimulating growth factors. TB 500 and BPC 157 together add the systemic piece: cellular migration, angiogenesis, and stem cell mobilization. The two mechanisms aren’t redundant. They’re sequential and complementary: BPC-157 initiates and directs the repair process, while TB-500 builds the vascular and cellular infrastructure that makes that repair sustainable.
This is why the BPC 157 TB 500 blend format exists. Rather than managing two separate vials, reconstitution processes, and dosing schedules, a pre-combined blend delivers both compounds in a single injection at a fixed ratio. We offer the Wolverine Stack as a pre-made combination specifically because the mechanistic case is so established – it’s not a marketing convenience, it’s a genuinely well-supported pairing.
BPC 157 TB 500 stacking is particularly effective for: post-surgical recovery where both local and systemic repair support is needed, chronic tendinopathies that haven’t responded to single-compound approaches, athletes returning from overuse injuries, and anyone where the injury involves compromised circulation to the affected tissue.
For broader coverage that goes beyond connective tissue, TB-500 is also part of both our GLOW and KLOW blends – in GLOW alongside GHK-Cu and BPC-157 for aesthetic and regenerative protocols, and in KLOW alongside KPV and GHK-Cu, where gut inflammation and systemic recovery are the primary focus.
Should You Stack or Run Them Separately?
The case for single-compound first is straightforward: you know what’s working. If you run BPC 157 TB 500 blend from day one and see improvement, you have no visibility into which component is driving it – or whether you even need both.
Starting with BPC-157 alone makes sense when the injury is specific and localized (e.g., a single tendon, a gut issue, or a single affected joint). If you reach week 4-6 with partial but incomplete improvement, TB-500 added as a systemic layer is the logical next step.
Starting with the BPC 157 TB 500 blend from the beginning makes sense for chronic multi-site injuries, post-surgical recovery involving multiple tissue types, or when the healing timeline is the primary constraint, and you want both mechanisms working from the start.
Advanced protocols sometimes run BPC-157 daily plus TB-500 2-3x weekly as separate injections for independent dose control. The pre-made blend is the simpler route for most researchers.
Final Verdict: Which Healing Peptide Is Right for You?
Both TB 500 peptide and BPC-157 deserve their reputations as the leading peptides for healing in research circles. They earned those reputations through different mechanisms and shine in different contexts.
BPC-157 for localized, acute injury and gut issues. TB-500 for systemic, chronic, or circulatory-limited injury. TB 500 benefits – cellular migration, angiogenesis, stem cell mobilization – are most pronounced exactly where BPC-157’s localized mechanism has limits. And the BPC 157 and TB 500 combination is the most comprehensive recovery stack in the peptide space for a reason: the two mechanisms cover each other’s gaps.
TB 500 side effects are minimal when the product is clean. Sourcing matters as much as the compound. Batch-tested, COA-verified peptides from verified vendors aren’t optional infrastructure – they’re what separates a research protocol that reflects the published literature from one that’s introducing unknown variables.